Lysosomal storage disorders are divided into several categories which include sulfatidosis, spingolipidosis, mucopolysaccharidoses, and glycogenosis among others. This article features the different types of mucopolysaccharidoses and the enzyme deficiency of each type.
Role of Lysosomal Enzymes in Lysosomal Storage Disorders
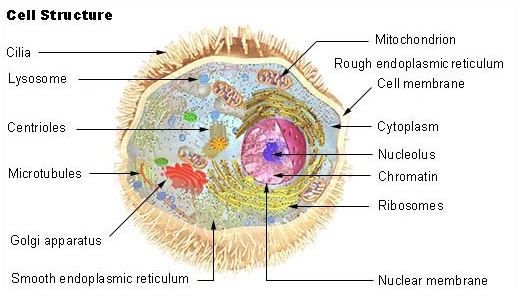
Lysosomes are organelles that are referred to as the recycling centers of cells. They contain specific enzymes that degrade proteins, carbohydrates, lipids and nucleic acids. Malfunction of these lysosomal enzymes gives rise to a group of conditions called Lysosomal Storage Disorders. All of them are inherited in an autosomal recessive pattern except for Fabry disease and Hunter syndrome, which are X-linked.
In lysosomal storage disorders the materials inside the lysosomes are not completely digested. They accumulate in the cell which leads to its enlargement. As a consequence, there is cellular dysfunction and the clinical manifestation of the disease ensues mostly during early childhood.
Types of Mucopolysaccharidoses
Mucopolysaccharidoses or MPS are a group of inherited disorders which are caused by enzyme dysfunction or missing enzymes that are required to break down carbohydrates called glycosaminoglycans. If these sugar molecules are not broken down they accumulate inside cells and tissues.
This group of disorders is characterized by multiple organ involvement, including the spleen, liver, blood vessels, bone marrow, lymph nodes and the heart. Patients often show joint stiffness, mental retardation and coarse facial features.
There are seven types of mucopolysaccharidoses.
MPS type I-H, or Hurler syndrome; MPS type I-S, or Scheie syndrome; and MPS type I-H/S, or Hurler-Scheie syndrome, are all associated with a deficiency in the enzyme called alpha-L-iduronidase, with the accumulation of Herapan sulfate and Dermatan sulfate inside the cells. Patients manifest with mental retardation, coarse facial features, joint stiffness and corneal clouding as well as involvement of the heart, liver and spleen.
MPS type II, or Hunter syndrome, has a deficiency in Iduronate sulfatase leading to the accumulation of heparan sulfate and dermatan sulfate. Mental retardation occurs, but milder compared to Hurler syndrome. Patients manifest with retinal degeneration, coarse facial features, joint stiffness and pebbly skin lesions.
MPS type III has four subtypes which leads to the accumulation of heparan sulfate leading to severe mental retardation as well as coarse facial features in patients. They are:
- MPS III A, or Sanfilippo syndrome A, with enzyme deficiency of Heparan sulfamidase
- MPS III B, or Sanfilippo syndrome B with enzyme defect N-acetylglucosaminadase
- MPS III C, or Sanfilippo syndrome C, with involvement of enzyme N-acetylglucosamine 6-sulfatase
- and MPS III D, or Sanfilippo syndrome D, with enzyme defect N-acetylglucosamine-6-sulfate sulfatase
MPS type IV, or Marquio syndrome, with defect in enzyme Galactose 6-sulfatase, with the accumulation of Keratan sulfate and Chondroitin 6-sulfate. Patients manifest with corneal clouding, skeletal deformities and aortic valve defects.
MPS type VI, or Marotaeux-Lamy syndrome, with a deficiency in enzyme Arylsulfatase B, leading to the accumulation of Dermatan sulfate. The disorder manifests with corneal clouding, coarse facial features, valvular heart defects and skeletal deformities.
MPS type VII, or Sly syndrome, with defect in enzyme B-glucoronidase leading to the accumulation of Dermatan sulfate and Heparan sulfate. Liver enlargement is often present, as well as skeletal deformities, corneal clouding and mild mental retardation.
Treatment for Mucopolysaccharidoses
There is no cure for mucopolysaccharidoses at the present time. Patient management focuses on the treatment of symptoms and in the improvement of quality of life. Use of enzyme replacement therapy in MPS patients has proven to be promising. Many clinical trials investigating possible treatments for MPS are still ongoing.